About the Blog Author-John R. Hughes, MD
John R. Hughes, MD is Professor of Psychiatry, Psychology and Family Practice at the University of Vermont. Dr. Hughes is board certified in Psychiatry and Addiction Psychiatry. His major focus has been clinical research on tobacco use. Dr. Hughes received the Ove Ferno Award for research in nicotine dependence and the Alton Ochsner Award Relating Smoking and Health. He is a co-founder and past president of the Society for Research on Nicotine and Tobacco, and the Association for the Treatment of Tobacco Use and Dependence. Dr. Hughes has been Chair of the Vermont Tobacco Evaluation and Review Board which oversees VT’s multi-million dollar tobacco control programs. He has over 400 publications on nicotine and other drug dependencies and is one of the world’s most cited tobacco scientist. Dr. Hughes has been a consultant on tobacco policy to the World Health Organization, the U.S. Food and Drug Administration, and the White House. His current research is on how tobacco users and marijuana users stop or reduce use on their own, novel methods to prompt quit attempts by such users, whether smoking cessation reduces reward sensitivity and whether stopping e-cigarettes causes withdrawal. Dr Hughes has received fees from companies who develop smoking cessation devices, medications and services, from governmental and academic institutions, and from public and private organizations that promote tobacco control.
News
-
About the Blog Author-John R. Hughes, MD
John R. Hughes, MD is Professor of Psychiatry, Psychology and Family Practice at the University of Vermont. Dr. Hughes is board certified in Psychiatry and Addiction Psychiatry. His major focus has been clinical research on tobacco use. Dr. Hughes received the Ove Ferno Award for research in nicotine dependence and the Alton Ochsner Award Relating Smoking and Health. He is a co-founder and past president of the Society for Research on Nicotine and Tobacco, and the Association for the Treatment of Tobacco Use and Dependence. Dr. Hughes has been Chair of the Vermont Tobacco Evaluation and Review Board which oversees VT’s multi-million dollar tobacco control programs. He.. -
The ugly relapse curve
A while ago I published a paper describing the relapse curve in self-quitters (Addiction 99:29) showing most smokers cannot even remain abstinent f... -
Recent Cochrane Reviews
This year Cochrane updated 5 reviews. It is important to note that all of these were based on those already motivated to quit and did not assess the ability of the intervention to prompt new quit attempts.
The 75 studies of print-based self-help materials found that non-tailored materials had almost no benefit but tailored materials did (RR= 1.3) but these tailored benefits were also more intense. I would note that the Cochrane review on internet and social media treatments has not been recently..... -
Comment on the John Hughes, MD blog
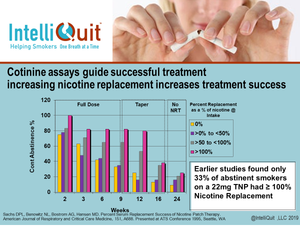
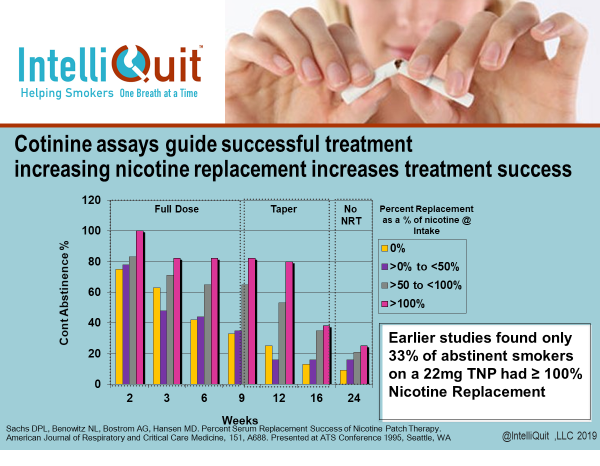 At SRNT last week (February 22, 2019) I presented data that parallels John's Blog. Almost 25 years ago, Sachs & Benowitz et al. reported on a study where they took smokers and measured their cotinine levels while smoking normally. They then assigned those subjects to nicotine patch replacement in quartiles from 0% replacement to 100% replacement or more. Not surprisingly, those with the highest nicotine replacement attained the highest levels of continuous abstinence from 100%....
At SRNT last week (February 22, 2019) I presented data that parallels John's Blog. Almost 25 years ago, Sachs & Benowitz et al. reported on a study where they took smokers and measured their cotinine levels while smoking normally. They then assigned those subjects to nicotine patch replacement in quartiles from 0% replacement to 100% replacement or more. Not surprisingly, those with the highest nicotine replacement attained the highest levels of continuous abstinence from 100%.... -
How effective is internet treatment? Should we replace or add to our in-person/quitline programs?
Currently, 77% of Americans have a smartphone and 88% have daily access to the internet via computer or smart phone, with only a slightly lower prevalence in smokers. The major advantages of e-therapy are easy access, affordability and reach.
A recent meta-analysis (Do et al, Patient Preference and Adherence 2018:12, p 2065) examined 108 (!) internet studies, most of which were those using text messages. E-therapy using the internet increased quit success by 70-80% (i.e., from about 10% to 15%). However, these maybe over-estimates as.... -
Tobacco Treatment Specialists Are Needed
In prior blogs on 11/2/04, 1/31/13 and 12/21/15 (see ATTUD website) I presented evidence on whether TTSs achieve quit rates greater than brief advice or Quitlines. One important study that I missed should be added to those reviews (Kotz et al, Addiction 109:491, 2013). This study used a survey of UK smokers. It is important for two reasons. The UK is the only country with lots of TTSs. And this study examined many more confounders (e.g. that those seen... -
Partner Support for Smoking Cessation
A recent Cochrane Review (“Enhancing Partner Support... 2018) concluded that the 11 RCTs indicate providing partner support to smokers trying to quit does not increase quit rates. There are multiple lines of evidence that partner support is associated with greater quitting. For example, living with another smoker decreases quit rates and if a smoker quits, his/her partner is more likely to later quit. Also, having a partner who is an ex-smoker increases quit rates, even more than having a never-smoker partner. Increasing partner support has been found effective for weight loss, diabetes compliance, and alcohol/drug abuse.... -
Is Marijuana Legalization Increasing Tobacco Use?
The title of a recent article stated that smoking is actually increasing over time in those using illegal drugs (Addiction 113:719). But when I read it, found that it was more complicated than that. Seems that cigarette use in those with opioid, cocaine, etc. dependence increased over time from 61% in 2002 to 68% in 2014 (ie.by 0.6%/yr.). But then smoking in those with cannabis dependence (which is 6 times more common) was decreasing over time at a rate even greater.... -
How Clinical Trial Statistics Can be Misleading
A recent review paper (Rosen et al, Addiction, in press) quantified how some cessation statistics can be misleading. Let’s see if I can summarize that without too much jargon.
The most commonly reported effectiveness statistics are the Odds Ratio (OR) and Relative Risk (RR). They are usually very similar and... -
Pre-dosing medications to increase efficacy
Recent studies on pre-dosing suggest it does, in fact, increase quit rates. Most studies of pre-dosing had participants use nicotine gum for about 4 weeks prior to the quit date and most did not ask smokers to try to reduce, but just smoke as usual. The idea is that with extra nicotine in the system, they would be tolerant and find nicotine via cigarettes less rewarding. Sort of like giving someone an IV drip of sugar will decrease food intake. The most recent Cochrane review on nicotine replacement therapy concluded that predosing increases quit rates by about 30%, including a very recent real-world trial ... -
Does the Addiction/Brain Disease Model Help or Hinder Tobacco Treatment
I and others have often tried to decrease “cessation fatigue” by decreasing self-blame of those who have failed to quit on multiple occasions (e.g. via having smokers believe that their inability to quit may not derive from poor willpower but due to a surplus of the addiction “disease”. But is this an evidence-based strategy?
The alcohol and illicit drug abuse treatment and research community has mostly believed that the “disease model” has been helpful. However, recent reviews suggest this may not be the case (Social Science and Medicine 96:95;... -
Tobacco use vs Cigarette use
An analysis of the large PATH survey reports that 26% of US adults are current tobacco users and 18% are cigarette smokers (NEJM 376:342, 2016). Thus, 1/3rd of tobacco use is from products other than cigarettes. The two most common non-cigarette tobacco products in the study were cigars (7%) and ecigs (5%).
A major question now becomes is what is our goal with treatment: abstinence from cigarettes (clearly the most harmful), abstinence from the more harmful combustible....


- Page 1 of 5
- Next page